Chiari Malformation
Chiari Syndrome Considerations for TAP
Chiari Syndrome, or Cerebellar Tonsillar Ectopia (CTE) is a condition where one or both of the lowest anatomical parts of the cerebellum, the cerebellar tonsils, drop down, and move away from their normal positions inside the occipital skull-base. As they drop out of their normal station inside the skull-base, they begin to encroach upon the other vital tissues and fluids that must pass through the great opening in the center of the craniocervical junction. This opening is known as the Foramen Magnum, which simply means “big opening”. One of the primary aspects of chiari, or cerebellar tonsillar ectopia is the low-lying cerebellar tonsillar presentation visible on MRI. This tonsillar ectopia causes the disruption of cerebrospinal fluid through the canal, and restriction of arterial and venous blood in the vessels at the level of the tonsillar blockage, which is always identified at the foramen magnum, the upper opening of the craniocervical junction. As the tonsils descend, the cerebellar tissue and brainstem matter converge due to the shape of the canal, and compress more tightly together in the funnel-shaped craniocervical canal. This convergence of brain tissues under pressure, along with restrictions in the healing flow of cerebrospinal fluid, produces many of the chronic symptoms associated with Chiari and/or low-lying cerebellar tonsils.
CSF flow disturbances negatively affect all brain and brainstem function, making every other malady more intense and insufferable. When the corking effect is present, it prevents complete recovery of injured and diseased brain tissue and adds to the overall “feeling of not being well” often expressed by those who suffer from chiari syndrome. The reason CSF flow is so critical is because in one important way, the brain is like a sponge. It holds debris and waste particles in its own tissues until those wastes can be cleared through the convective movement of cerebrospinal fluid and interstitial fluid. If CSF is not flowing, because its pressure cannot overcome the tonsillar blockage, the waste products then accumulate in the very small but wonderfully abundant spaces around all brain cells, and begin to build up in the tissue. Just like a dirty sponge that needs a good rinsing.


The brain holds wastes like a sponge until spinal and interstitial fluid clears it out, moving it into the venous sinuses and out the internal jugular veins and venous plexuses of the skull!
New research is linking the build up of these “un-cleared” bi-products of brain metabolism to a variety of neurodegenerative brain diseases. Since movement of spinal fluid into and out of the skull is the key factor that powers the pressure gradients that drive the glymphatic system (the brain’s own special version of a lymphatic system), waste products begin to build up and the brain tissue becomes unhealthy as this vital clearance system loses optimal function.
In a low-lying cerebellar environment, the cerebellar tonsils descend into the opening at the junction compressing blood vessels and the brainstem. This phenomenon behaves like a cork stop in a bottle. Because it mostly corks the movement of cerebrospinal fluid from entering the skull, which occurs rhythmically, in cadence with diaphragmatic inspiration. As the diaphragm drops down, thoracic pressure becomes more negative than the atmosphere and the intracranial environment. The contents inside the pericardial sac (including the heart) draws down venous blood from the internal jugular veins, which in turn pulls the venous blood out of the venous sinuses towards the right side of the heart. This thoracic pressure allows CSF to favor upwards movement through the foramen magnum into the skull. The draw on the venous side augments the siphoning of CSF upwards and creates the conditions that drive the convective movement of CSF through the brain tissue. This is why unobstructed breathing is so critical to brain health, and why breathing obstructions can secondarily deprive the brain of being cleaned by this vital upward fountain of nutritive and cleansing cerebrospinal fluid.


Top View of low-lying cerebellar tonsils (red arrows) corking the spinal column
and the same view of a cork in a bottle
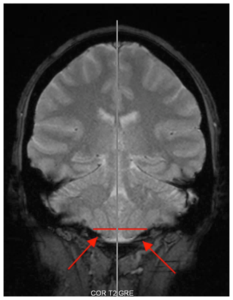

Front View of low-lying cerebellar tonsils (red arrows) corking the spinal column
and the same view of a cork in a bottle
While this condition sounds life-threatening, and can be in its more severe aspects, most individuals who suffer from cerebellar tonsillar ectopia or chiari manage their symptoms by taking pharmaceutical drugs, or through invasive, decompressive surgeries.
A word about surgeries, from a non-surgeon.
Often the drugs stop working, and surgical outcomes rarely resolve all symptoms, and often can create additional symptoms.
Moreover, many ectopic cerebellar tonsils fall outside of conventional chiari surgical guidelines. One of those guidelines considers how low the tonsils have descended through the foramen magnum into the neural canal where the brainstem and other important structures are located. For instance, if the cerebellar tonsils do not descend “low-enough” to operate, (usually 10mm is the standard), no surgery may be opted. That means that if the lowest presenting cerebellar tonsil was 1.5mm below the foramen magnum, you would not meet the criteria that factors into chiari decompression surgery. Even if the tonsils are, nonetheless, encroaching upon vital brain tissue and vessels, or more likely, suppressing CSF flow dynamics.
It’s helpful to remember that these guidelines exist for a reason. Risk. It is a risky surgery, and the potential benefits of a dangerous operation need to outweigh all of the symptoms. Surgical procedures have come far since the first decompression surgery was performed, but the risks of neurosurgery are considered high, because… . Well, it’s brain surgery. Transdermal Atlas Positioning is another safe option that can radically improve your quality of life if you suffer from chiari and/or cerebellar tonsillar ectopia.
Transdermal Atlas Positioning (TAP) has helped many suffering from Cerebellar Tonsillar Ectopia, or low-lying cerebellar tonsils, including storied NFL quarterback, Jim MacMahon. He reported that it felt like a toilet flushed at the bottom of his brain as his headache disappeared.
TAP has helped many with low-lying cerebellar tonsils who have already been diagnosed and medically treated for chiari malformation or low-lying cerebellar tonsils. Essentially, the TAP procedure re-aligns the funnel shaped canal from the occipital foramen magnum to C3, and this alignment helps the cerebrospinal fluid move more normally in and out, depending on the cycle of breath, and whether you are upright or recumbent. Most symptoms start to improve or resolve immediately.
We can achieve these results even if you are post-surgical, currently treating with meds, or considering surgery as an option. Or, if you think you might have low-lying cerebellar tonsils or chiari after reading our list of symptoms, but haven’t yet been diagnosed, we can help diagnose and often treat mild to severe forms of chiari and cerebellar tonsillar ectopia.
We are always happy and willing to collaborate with your other health care providers as you find your way to recovery and good health. We encourage you to set up a consultation today, because sometimes all you need to do is pop the cork!

Request Consultation
Fill this out and we will be in contact with you
"*" indicates required fields
